


Indirect Evidence of Death by Vaccine
Citing an academic article based on German all-cause mortality

Truth was the first casualty in the war on COVID. Trusted sources of medical information became propaganda outlets, and when that wasn’t enough, the raw data on which medical analysis was based was withheld and even falsified by the governments that controlled it.
All along, we have been piecing together indirect evidence. It paints a picture of a devastating toll from vaccine injuries in the last year. No drug product in the past has been anything like this. Injuries from the worst vaccines have come in at a rate about 1/100 of the mRNA vaccines. Thalidomide maimed tens of thousands of babies compared to 1.4 million vaccine injuries and 30,000 deaths in the last year and a half, counting only those that were reported to VAERS, the CDC’s Vaccine Adverse Events Reporting System. The only comparable drug disaster was oxycontin, which led to about 20,000 overdose deaths in its worst year.
The evidence is radioactive. No one in government wants to count up the deaths and injuries because of the political ramifications. Most medical researchers, even at universities, are dependent on money from NIH and the drug industry.
Hence, it’s refreshing to see an honest analysis of apparently honest government data. The analysis comes from Christof Kuhbandner and Matthias Reitzner, professors of sociology and mathematics, respectively, at two German universities. The data is from the German Federal Statistical Office (Bundesamt für Statistik). I’m grateful to a fellow Substacker who writes under the pseudonym Eugyppius for calling my attention to this article and placing it in context.
Of course, what we would like to have is a count of deaths and hospitalizations due to COVID and corresponding counts for deaths and hospitalizations due to the vaccines. This data has been disguised or deleted by governments around the world. The very definitions of causality have been gamed for these two cases.
Draw your own conclusions.
But data on all-cause mortality are more difficult to disguise or to reinterpret, as our two authors are quick to point out. This is a simple list of people who died, together with their age and sex, and no overlaid story about how they met their demise.
The point is that we can find patterns in this data that hold implications for COVID epidemiology and COVID policy.
Take-home Message
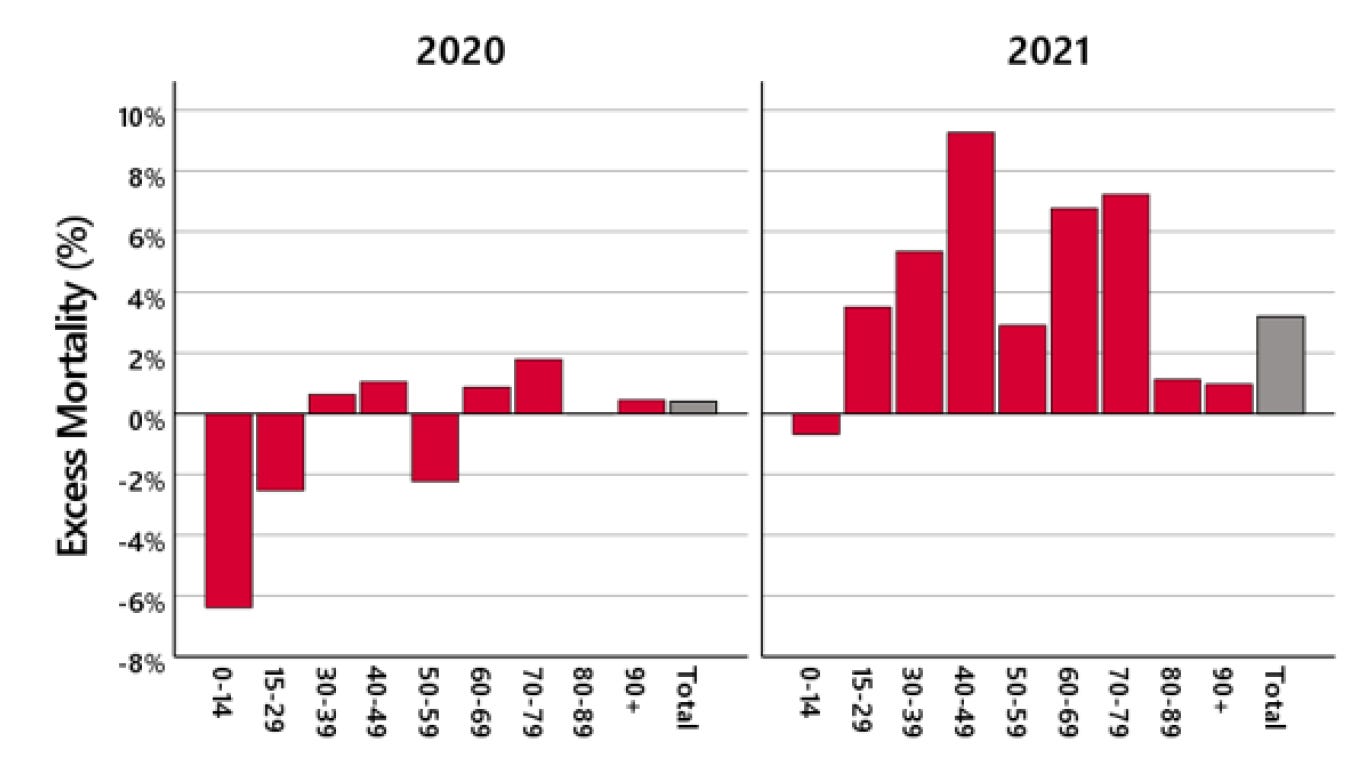
Here’s the bottom line: In 2020 Germany, we see a slight excess of death in the oldest age group, too small to be significant. In 2021, we see a large excess of death in young and middle-aged people.
What happened in 2021 that made it different from 2020? In both years, we had COVID. We expect the second year of a pandemic to be milder than the first, based on past experience. In both years we had lockdowns and deaths of despair, but again, the lockdowns were more severe in 2020 compared to 2021.
The elephant in the room is the vaccine campaign. In Germany, as in the US, there was a big propaganda push urging people to accept the experimental, hastily-tested vaccines. In Germany, as in the US, there was coercion by employers and public venues.
The authors of the academic paper stick to “just the facts, Ma’am”. Except for one understated paragraph, they never use the word “vaccine”. But they demonstrate that, whatever it was that started killing young, healthy people, it began in April, 2021.
Vaccination began in December, 2020, with front-line medical workers and the elderly. For younger, working people, the time when vaccination began in earnest was April, 2021.
But correlation is not proof of causation, so draw your own conclusions.
Statistically, we see the results jump out at us most clearly for young people. Does that mean that the vaccines are less likely to injure the elderly? Not necessarily.
Among healthy middle-aged people, the baseline death rates are quite low, so that the vaccine’s contribution to mortality expressed as a percentage sticks out more prominently, even though the absolute numbers are not as large as the count of old people killed by the vaccines.
Governments and their mouthpieces in the media would like to attribute the 2021 excess deaths to COVID, but we know that COVID deaths are heavily concentrated in the oldest age range, and what happened in 2021 did not fit that pattern.
Details
I recommend the journal article as exceptionally readable and even-handed. The authors review other analyses of patterns in all-cause mortality. They point out that we are interested in departures from past trends, but there is no way to define those trends objectively.
To account for past trends quantitatively requires a computer model, and as we know, there are many ways to construct a computer model.
There are four moving parts to be accounted:
Overall population is increasing
Overall death rates are decreasing
The proportions of the population in each age group are changing
The mortality rates of these different subpopulations were already changing before COVID
The authors both acknowledge the strengths of previous analyses and note the places where one or more of these four adjustments were not part of the calculation. They then proceed to their own analysis, based on actuarial tables. You may already be familiar with how actuarial tables work. They are used to calculate insurance risk, and typically they list probabilities of death for a one-year period, based on age, sex, and sometimes race.
(Insurance companies are motivated to make a profit, and they don’t mess around with fudge factors. That’s why it was so alarming when a number of insurance companies announced earlier this year that their group life policies had paid out higher benefits in the last half of 2021 at an unprecedented level.)
The authors track the trends in actuarial tables from the past several years and use them to construct tables for Germany in 2020 and 2021. They combine these with census data for the number of Germans in each age group to create their estimates of how the actual number of deaths differed from expectations. That is the methodology that went into the graph above.
The database they use also includes dates for each death. The authors were able to track when in time the excess deaths among 30-79 year-olds occurred. The answer: The excess deaths began in April 2021 and continued through most of the year. Deaths for the age range 60-79 were up 20%, April 2021 thru March 2022.
A simpler approach
Most of the effort and the technical detail in the article is devoted to defining an expected mortality rate for each age group. But for what we want to know, this is largely unnecessary. We can simply compare 2020 with 2021.
2020 — this is what mortality looks like with COVID
2021 — this is what mortality looks like with COVID + vaccines

In every age group, mortality was higher in the year of the vaccine. Isn’t that all we really need to know?
Here’s the corresponding graph, computed with CDC data for the USA:

The US data are qualitatively similar to Germany, but there are some differences which have no obvious source. The percentage increases for young people are about twice as high in the US. But for people over 75, there is actually a net decrease in mortality in the US (but not in Germany).
We will continue to piece together the story
Independent researchers around the world will continue to analyze evidence of the scope of injuries and deaths from the mRNA vaccines. Direct evidence is not being collected, or it is being withheld by governments around the world. But the extent of the damage has been so devastating that it cannot be hidden. Everyone you know has had friends or relatives injured by the vaccines. I will continue to monitor the research outlets in our ongoing efforts to quantify the damage, and I will report what I find on this web page.
I've read the report through quickly and one of the observations was for the increase in stillbirths. The definition was changed in 2019 from baby delivered weighing over 500 gr to that plus 24 weeks gestation and authors say this would increase numbers but in comparison to 2019, 2020 showed no increase but shows ave 10% increase since. The miscarriages happening in first trimester must therefore be accounted for in the much lower live birth figures. I hope and pray that no permanent damage has been done to these women.
Is the spike protein acting as a prion with regard to hemoglobin molecules? And is porphyria being induced?
If the answers are 'yes', this is very bad news.
--
Here’s a key paragraph from that article:
So the bottom line of all of this information is this: the virus infects the RBCs using spike protein via the CD147 receptor on red blood cells which causes hemolysis (rupture of the red blood cell). This causes the release of massive amounts of hemoglobin. Then the spike protein, due to its amyloidogenic peptides, triggers mis-folding of the hemoglobin into amyloid fibrils causing subsequent blood clots. The blood clots would be enhanced due to antibodies (Ag:Ab complexes).
https://jessicar.substack.com/p/is-the-spike-protein-acting-as-a